IntraLase History - Advancement in LASIK Technology
Advancement in LASIK technology
In our blog posts we have looked at IntraLase and the femtosecond laser, but we have only scratched the surface of the development of this advancement in LASIK technology. And that word “advancement,” ahh… throughout the history of science, humankind has seen practical instruments, methodologies, and theories giving way to new ones as the old ones no longer “work.” Indeed, the science of laser vision correction has its history, too, and very specially when in comes to IntraLase, a perhaps “miraculous” technological advancement from the microkeratome.
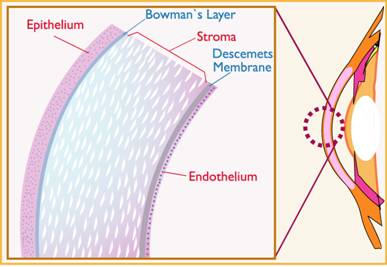
Soon after the discovery in 1980 of the excimer laser’s possible application to vision correction, there was another step yet to be taken before the excimer could perform its function in the LASIK procedure. The excimer laser had to be applied to the corneal stroma, which is the layer of tissue just beneath the surface layer, or corneal epithelium. This surface layer of the cornea had to be lifted up, like a flap, preserved during the excimer laser step, and then be laid back down onto the laser-treated stroma.
How to create this flap? The first method was to do it with a scalpel-like metallic instrument—the aforementioned microkeratome (invented in the 1950s), which makes a circular incision, creating a flap, with a hinge or small segment left connected to the epithelium or surface layer of the cornea.
Microkeratome’s Performance Problems
Several problems arose with the microkeratome’s performance of this step, however, as follows. The microkeratome’s flap-making became the main source of vision-threatening complications in the LASIK procedure—in the form of (1) free caps (unattached flaps—no hinge), (2) partial flaps, (3) buttonholes (improperly formed flaps), or (4) an epithelial slough (damaged eye tissue).
Surgeons reported that even though the vast majority of LASIK procedures using a microkeratome went well, when they didn’t go well it was serious.
Introducing IntraLase
Then, when the FDA approved the IntraLase laser flap maker, in 1999, many surgeons found the IntraLase to alleviate the problems they had been having with the microkeratome.
One of the big improvements is that the IntraLase creates a corneal flap of uniform thickness, whereas the microkeratome flap is always thinner at the center, making it liable to tear—hence the “buttonhole” flap. Moreover, with the microkeratome blade, the more curved a patient’s cornea is, the thinner the center of the flap will be, increasing the chance of a buttonhole tear significantly. The beauty of the IntraLase in this regard is that the femtosecond laser creates a layer of bubbles at a uniform distance beneath the epithelium, for the entire area of the flap, whereby the thickness of the flap is the same wherever it could be possibly be measured—at the center, the edges, corners, etc.
Some LASIK surgeons still use the microkeratome, and it is up to the prospective LASIK patient to be fully informed on the difference between the microkeratome and IntraLase, and choose wisely.
Image source: http://www.hybridcornea.org/aboutcornea.htm
Image source: www.operationauge.de


